Clinical Features and Diagnosis of Subdural Haematoma (Head Injury):
 Subdivision of subdural haematomas into acute and subacute forms serves no practical purpose. Chronic subdural haematoma however is best considered as a separate entity, differing both in presentation and management.
Subdivision of subdural haematomas into acute and subacute forms serves no practical purpose. Chronic subdural haematoma however is best considered as a separate entity, differing both in presentation and management.
- Chronic subdural haematomas – fluid may range from a faint yellow to a dark brown colour.
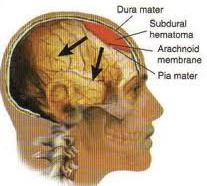
- A membrane grows out from the dura to envelop the haematoma.
- Chronic subdural haematomas occur predominantly in infancy and in the elderly. Trauma is the likely cause, although a history of this is not always obtained.
Predisposing factors
- Cerebral atrophy
- Low CSF pressure (after a shunt or fistula)
- Alcoholism
- Coagulation disorder
Breakdown of protein within the haematoma and a subsequent rise in osmotic pressure was originally believed to account for the gradual enlargement of the untreated subdural haematoma. Studies showing equality of osmotic pressures in blood and haematoma fluid cast doubt on this theory and recurrent bleeding into the cavity is now known to play an important role.
Clinical Features
- Dementia.
- Deterioration in conscious level, occasionally with fluctuating course.
- Symptoms and signs of raised ICP.
- Focal signs occasionally occur, especially limb weakness. This may be ipsilateral to the side of the lesion, i.e. a false localising sign.
Diagnosis
- CT Scan appearances depend on the time between the injury and the scan.
- With injuries 1-3 weeks old, the subdural haematoma may be isodense with brain tissue. In this instance, i.v. contrast enhancement may delineate the cortical margin.
- Beyond 3 weeks subdural haematomas appear as a low density lesion.
Adult
- The haematoma is evacuated through two or three burr holes and the cavity is irrigated with saline. Drains may be left in the subdural space and nursing in the head-down position may help prevent recollection.
- Craniotomy with excision of the membrane is seldom required.
- In patients who have no depressed conscious level, conservative treatment with steroids over several weeks may result in resolution.
Infants
The haematoma is evacuated by repeated needle aspiration through the anterior fontanelle. Persistent subdural collections require a subdural peritoneal shunt. As in adults, craniotomy is seldom necessary.
Braner Pain Clinics specialize in chronic pain management, neurology, neurological testing and disability. Our clinics are conveniently located in Northern Virginia minutes away from Interstate 495 (Beltway). Call today at: (703) 573-1282
Visit Our Website: http://www.branerpainclinic.com
